
Ventilator modes
I think I need some pressure support to understand this

Ventilator Settings
Mechanical ventilators and their modes have become increasingly complicated in recent years and can vary among brands. The following are the basic modes used in most intubated patients:
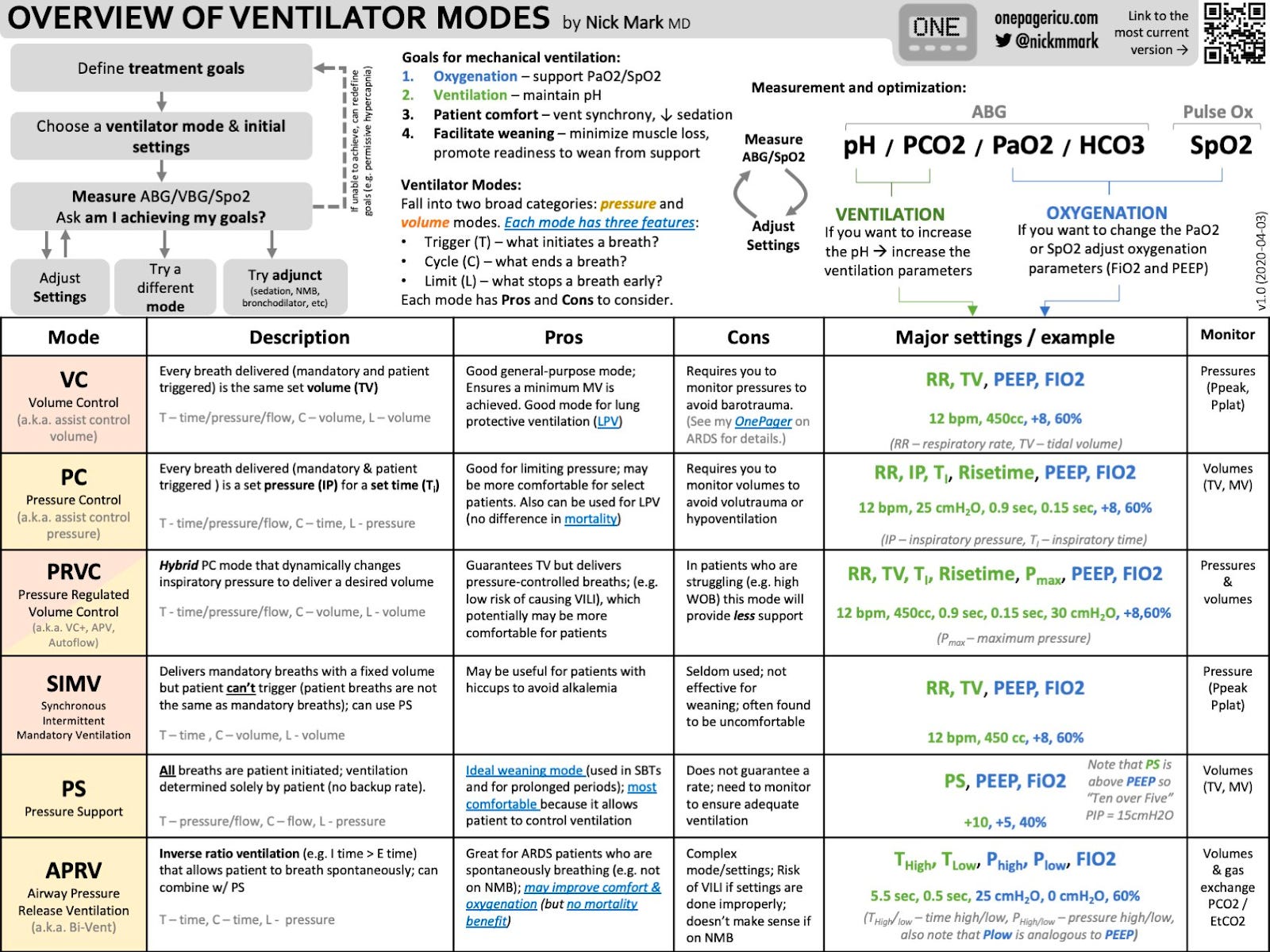
Assist–control ventilation (AC)/continuous mandatory ventilation ventilator sets the fraction of inspired oxygen (FiO2) and a minimum respiratory rate (patient can trigger more); ventilator supports all breaths with either volume or pressure cycling as follows:
volume-controlled (VC): set tidal volume; ventilator delivers breath until set tidal volume is reached (end-inspiratory pressure varies with lung compliance)
benefits: more control over ventilation, best for ARDSNet ventilation (see ARDS in this rotation guide)
drawbacks: ventilator–patient dyssynchrony (i.e., patient does not synchronize their breathing with the ventilator cycle), risk of lung injury from high airway pressures due to dyssynchrony
as a safety feature in the VC mode, most ventilators either stop the inspiratory gas flow when the “cutoff pressure” is reached or change the delivery system such that gas is delivered for the remainder of the ventilatory cycle at the set pressure
Pressure-controlled (PC): set airway pressure; ventilator delivers breath until set pressure is reached (tidal volume varies with lung compliance)
benefits: variable flow during inspiration, less dyssynchrony
drawbacks: no guaranteed minute ventilation, unable to guarantee low tidal volume ventilation (see ARDS in this rotation guide)
Pressure support ventilation (PSV): for spontaneously breathing patients; used to wean from mechanical ventilation; delivers a set level of airway pressure (usually 5–15 cm H2O above positive end-expiratory pressure [PEEP] during inspiration) to augment spontaneous breath; patient controls duration, respiratory rate, and tidal volume
General Principles: how to manage
Titrate the ventilator settings to acceptable physiological parameters (i.e., some degree of hypoxemia and hypercapnia is acceptable).
Use low tidal volumes to avoid ventilator-induced lung injury.
Use the lowest fraction of inspired oxygen (FiO2) to maintain oxygenation at 90%–92%. Positive end-expiratory pressure (PEEP) can recruit collapsed lung units and improve oxygenation.
Some of the main settings we can change on the ventilator
In order to change oxygen levels of the patient
Fraction of inspired O2 (FiO2)
Positive end expiratory pressure (PEEP)
In order to change CO2 levels of the patient
Respiratory rate (RR)
Tidal volume (TV)
Which is better?
Every breath comes with some dead space. Dead space is that part of the respiratory circuit that does not play a part in gas exchange. The gas simply moves along these areas and gas exchange does not occur. Some of this is created by the ventilator tubing and some of it is physiological dead space.
If you increase the rate, then the ventilation of the patient will increase as every minute you are giving them additional breaths. The problem however is that you are also increasing the amount of dead space ventilation you are giving them, as each additional breath also carries the same amount of dead space. This process can increase the patient’s propensity to retain carbon dioxide.
Source: https://resident360.nejm.org/rotation-prep/critical-care/ventilation/fast-facts)

Source: @nickmmark